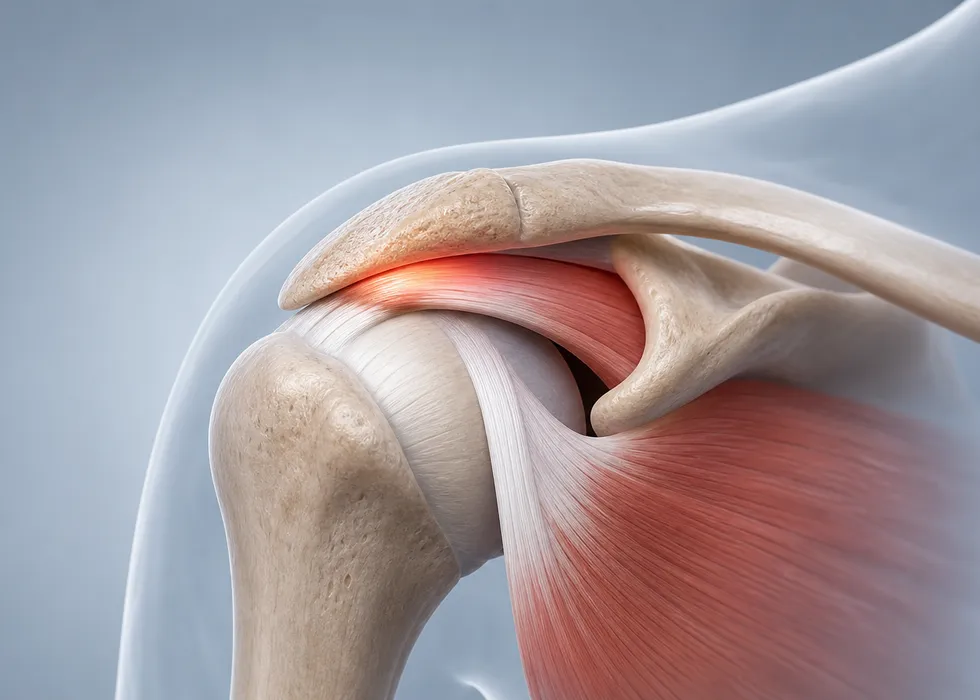
Shoulder impingement syndrome describes pain caused by repetitive mechanical conflict in the subacromial space, often involving the rotator cuff tendons, bursa, or surrounding structures. In practice, it is less a single diagnosis and more a biomechanical pain pattern with several possible causes.
Why It Happens
The shoulder depends on coordinated movement between the humerus, scapula, thoracic spine, and rotator cuff. When that rhythm is altered, structures in the subacromial space can become irritated. Contributing factors may include:
- Rotator cuff weakness
- Scapular dyskinesia
- Overhead activity
- Tight posterior capsule
- Structural narrowing or acromial shape
- Associated tendon degeneration
It is often seen in people who repeatedly raise the arm overhead, whether in sports, work, or daily activity.
Typical Symptoms
Patients usually describe:
- Pain when lifting the arm
- Painful arc during overhead movement
- Night pain, especially when lying on the shoulder
- Weakness or fatigue with repeated use
- Difficulty reaching behind the back or into a cabinet
If symptoms persist, secondary stiffness or compensatory movement patterns may develop.
Evaluation
The examination looks at range of motion, cuff strength, scapular control, and provocative maneuvers. Imaging may include radiographs to assess bone structure and ultrasound or MRI when tendon damage or other pathology is suspected.
It is important to distinguish impingement-type pain from other causes of shoulder pain such as adhesive capsulitis, instability, cervical radiculopathy, or full-thickness rotator cuff tear.
First-Line Treatment
Most patients improve without surgery when the treatment plan addresses mechanics rather than pain alone. Effective conservative care often includes:
- Activity modification
- Anti-inflammatory treatment when appropriate
- Rotator cuff strengthening
- Scapular stabilization
- Postural and thoracic mobility work
- Stretching of tight structures
The aim is to restore smooth shoulder mechanics so the irritated tissues are no longer repeatedly overloaded.
When Injection or Further Imaging Is Helpful
Subacromial injection may help selected patients with significant inflammation or persistent pain. It can reduce symptoms enough to allow better participation in rehabilitation. Imaging becomes more important when weakness is marked, trauma preceded symptoms, or conservative treatment is failing.
When Surgery Is Considered
If symptoms remain functionally limiting despite a structured rehabilitation program, surgery may be discussed. The exact procedure depends on the underlying pathology. In some cases, treatment focuses on cuff repair or other associated pathology rather than isolated decompression alone.
Practical Takeaway
Shoulder impingement is best understood as a movement and load-management problem. Many patients improve substantially when the diagnosis is made carefully and rehabilitation is matched to the real mechanical driver of pain.